Scan to BIM for healthcare renovation is the process of using laser scanners to capture the existing conditions of an occupied hospital, registering those scans into a unified point cloud, and modeling the point cloud in Revit to produce an accurate as-built BIM. The work has to be done without disrupting patient care, which means scanning during off-hours, working under ICRA infection control protocols, and phasing the capture wing by wing. The output is a federated as-built model that includes architectural, structural, MEP, medical gas, life safety, and medical equipment data, ready to support renovation design and construction.
This guide walks through why scan to BIM healthcare renovation is one of the hardest workflows in the scan-to-BIM space, what makes hospital scan to BIM different from standard commercial scanning, how to phase capture across an occupied facility, what an as-built hospital BIM should include, and how Eagle BIM delivers healthcare renovation modeling for Texas hospital systems. Written for hospital facilities teams, healthcare GCs, owner reps, and design firms working on renovations, expansions, and infrastructure upgrades to occupied healthcare buildings.
Why Healthcare Renovations Are the Hardest Scan-to-BIM Projects
Healthcare renovations are the hardest scan-to-BIM projects because hospitals never close. A retail tenant fit-out can scan empty rooms during normal business hours. A vacant office building can be scanned in a single afternoon with full access to every space. A hospital cannot. Patients are in beds, surgical suites are running, imaging equipment is operating, and infection control protocols govern every move. The scanning team has to work around all of it while still capturing the existing conditions accurately enough to support a renovation design that will be built two years later.
Scan to BIM healthcare renovation work happens in a constraint-rich environment that doesn’t exist in any other sector. Three constraints dominate. First, operational continuity: the hospital cannot pause patient care for scanning. Second, infection control: infection control scanning has to comply with ICRA (Infection Control Risk Assessment) protocols, which dictate everything from cart staging to dust containment to equipment cleaning between rooms. Third, data sensitivity: scan teams operate in spaces with patient information, monitoring equipment, and confidential clinical activity that cannot be captured in imagery.
Hospital renovations are also high-stakes. The renovation work that follows the scan typically involves system upgrades, expansion, or compliance work that has to be coordinated against an existing MEP infrastructure that’s often poorly documented. Old hospital drawings are notoriously incomplete. As-built drawings from prior renovations are often missing, wrong, or contradicted by the actual conditions. Healthcare renovation modeling depends on the scan-to-BIM team capturing what’s actually there, not what the original drawings claimed. Getting this wrong on the front end costs the construction team months of field RFIs on the back end.
Industry data from the
American Society for Health Care Engineering (ASHE) shows that more than half of US hospital construction spending now goes to renovation and expansion of existing facilities rather than new construction. As the installed hospital stock ages, §F§scan to BIM healthcare renovation§ has become a foundational capability that owners, GCs, and design firms increasingly require as a precondition to scoping any major renovation.
What Makes Hospital Scanning Different From Standard Scan to BIM
Hospital scanning differs from standard scan to BIM in three specific ways. First, infection control compliance during capture: scanners and operators have to follow ICRA Class III or Class IV protocols, including cart-mounted HEPA filtration, dust barriers when scanning above ceilings, and disinfection between zones. Second, working around 24-hour operations: capture happens during off-hours, weekends, and scheduled shutdowns, never during normal patient care hours in clinical areas. Third, scanning above existing ceilings to capture MEP routing: standard scanning captures what’s visible, but hospital renovations require above-ceiling capture which means above-ceiling access ports, lift trucks, and ceiling tile removal coordinated through facilities.
Infection Control Compliance During Capture
Infection control scanning is the single biggest discipline that separates healthcare scan-to-BIM from any other sector. The American Society for Health Care Engineering publishes ICRA guidelines that classify renovation activities by their risk to patient populations. Even a non-destructive activity like laser scanning falls under ICRA because the scan team is moving through occupied clinical zones with equipment that has to be disinfected between rooms. Scan teams working in hospital ICRA Class III and Class IV zones must follow specific protocols: HEPA-filtered cart staging at every zone entry, equipment cleaning between rooms, dust barriers when probes go above ceilings, and tracked entry/exit logs.
Scan to BIM healthcare renovation teams operate under ICRA protocols throughout the capture phase. Eagle BIM’s standard healthcare scan engagement includes a pre-scan ICRA coordination meeting with the hospital’s facilities and infection control leadership to walk every zone the scan team will enter, document the ICRA classification, and agree on protocols before any scanner enters the building. Skipping this step is how scan teams get locked out of buildings mid-project.
Working Around 24-Hour Operations
Hospitals run continuously. Patient rooms have patients in them at all hours. Operating rooms have surgeries scheduled around the clock. Emergency departments never close. The occupied building scan workflow has to accommodate this reality. Standard scan-to-BIM projects scan during business hours; hospital scan projects scan during the night shift, weekends, and pre-planned shutdowns. Patient floors typically scan after 10pm when patients are sleeping, surgical suites scan during scheduled cleaning windows or after the day’s case load wraps up, and imaging suites scan around the equipment’s daily downtime.
Capture timing has to be negotiated with charge nurses, surgical schedulers, and facilities operations weeks in advance. The scan team coordinates with the hospital’s clinical operations leadership to identify off-hours windows, coordinate room access, and adjust for last-minute schedule changes. This is fundamentally different from commercial scan-to-BIM, where the building is empty after 5pm and scanning is straightforward.
Scanning Above Existing Ceilings
Hospital scan to BIM work has to capture above-ceiling conditions because renovations almost always touch MEP infrastructure in the plenum. Above-ceiling capture requires removing ceiling tiles, deploying scanners or probes into the plenum space, and reinstalling tiles cleanly. In ICRA Class III and IV zones, this means dust containment, HEPA negative air filtration, and coordination with the hospital’s facilities team for tile removal and reinstall. Some healthcare scan-to-BIM teams use small probe-mounted cameras or compact scanners that fit through standard ceiling tile openings; Eagle BIM uses both full-scale scanning with deployed sensors and probe-camera capture depending on access conditions.
Above-ceiling capture is the difference between a scan-to-BIM deliverable that’s useful for renovation design and one that isn’t. Hospital renovation work almost always touches HVAC ductwork, plumbing risers, electrical conduits, fire protection mains, and medical gas piping running in the plenum. If the as-built model doesn’t show what’s actually up there, the construction team discovers the conflicts in the field, where the cost of resolution is at its highest.
Eagle BIM’s scan to BIM healthcare renovation teams plan above-ceiling capture into the original scope rather than treating it as an add-on. The capture plan identifies every above-ceiling access point during the pre-scan walk, documents which areas need probe-camera vs full-scanner coverage, and coordinates the tile removal schedule with the facilities team. The hospital’s facilities maintenance staff often have the keys (literally and figuratively) to above-ceiling access. A scan team that hasn’t done this coordination work in advance will end up either missing data or losing scan days waiting for access.
There’s also a specific challenge with hospital scan to BIM in newer facilities with concealed plenums. Some modern hospital designs use rated corridor ceilings, dense fire-rated assemblies, or rigid plenum partitions that limit visual access. Capture in these conditions requires either scheduled ceiling demolition windows (rare on occupied buildings) or specialty probe-camera deployment that captures imagery without removing major ceiling assemblies. The capture strategy has to flex to match what the building allows.
Phased Capture Strategy for Occupied Hospitals
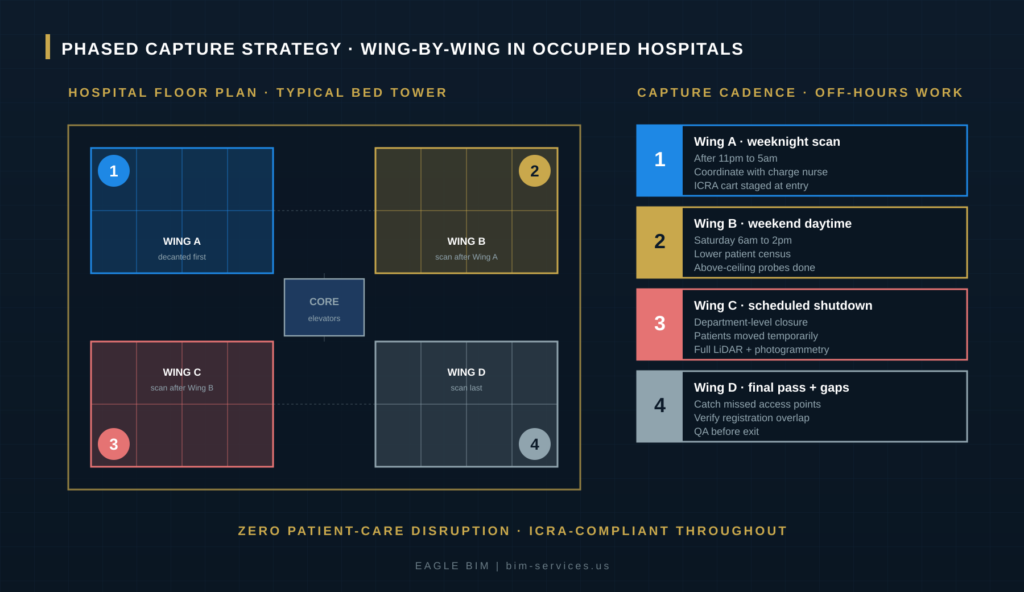
Phased capture for occupied hospitals divides the facility into wings or departments and scans each in sequence, coordinated to minimize patient-care disruption. Wing A scans first during weeknight off-hours when patient census is lowest. Wing B follows on a weekend daytime when activity is reduced. Wing C scans during a scheduled department-level shutdown if one is available. Wing D catches gaps and verification passes after the prior wings complete. The phasing typically takes four to twelve weeks total for a full bed tower, depending on facility size, patient census patterns, and how aggressively the hospital is willing to schedule short shutdowns.
After-Hours and Weekend Scanning Windows
Off-hours scanning is the primary tool in the scan to BIM healthcare renovation workflow. Most hospital floors are quieter from roughly 10pm to 5am: rounds are done, most patients are sleeping, fewer staff are present, and clinical activity is at its lowest. Scan teams enter the facility through coordinated entry points, set up equipment in pre-staged ICRA cart configurations, and work room by room through the wing during the quiet window. Each scan station takes 4 to 8 minutes for the actual capture plus setup and teardown time.
Weekend daytime scanning works for outpatient zones (clinics, imaging suites, ambulatory surgery centers) that have reduced or no operations on weekends. Procedure rooms and recovery zones in those areas can often be scanned during normal weekend hours without disrupting active patient care. Inpatient zones (med-surg floors, ICU, OR) almost always require off-hours or after-hours work because patients are present every day of the week.
Wing-by-Wing Capture Sequencing
Hospital floor plates are typically organized in wings around a central elevator and utility core. The occupied building scan workflow takes advantage of this geometry by scanning one wing at a time, leaving the others fully operational. Eagle BIM’s standard sequence starts with the wing scheduled for the heaviest renovation work, captures it first to give the design team the longest lead time, then moves through adjacent wings based on facility access constraints and patient census patterns.
Wing-by-wing sequencing also lets the scan team validate registration between wings as each phase completes. Registration targets placed along corridors connect the wings together, ensuring that the final point cloud aligns properly. Without disciplined sequencing and target placement, the wings drift apart in coordinate space and the as-built model loses accuracy at the wing-to-wing transitions, which is exactly where renovation work often happens.
Coordinating With Facilities and Infection Control
Every healthcare scan-to-BIM engagement starts with a coordination meeting that includes the hospital’s facilities team, infection control leadership, clinical operations, and the scan team. The agenda covers: zone classifications under ICRA, access protocols, after-hours entry coordination, equipment staging locations, dust containment requirements, above-ceiling access procedures, and the project schedule. This meeting is the gate before any scanner enters the building. Hospitals that have been burned by under-coordinated scan teams in the past will refuse access to any team that hasn’t done this prep work.
During the capture phase, the scan team’s daily workflow includes pre-shift briefings with facilities, real-time coordination with the night-shift charge nurse if working clinical areas, and exit debriefs that document any clinical activity that affected the planned scan zones. The point cloud healthcare deliverable depends on this discipline. A scan team that disrupts patient care or violates ICRA protocols on one project will not get a second chance, with that hospital or any other in the system.
| Need Scan to BIM for a Hospital Renovation?
Eagle BIM delivers scan to BIM healthcare renovation services across Texas and the USA for hospital owners, healthcare GCs, MEP subcontractors, and design firms. ICRA-compliant capture, phased wing-by-wing sequencing, and federated as-built models ready for renovation design. |
What an As-Built Hospital BIM Should Include
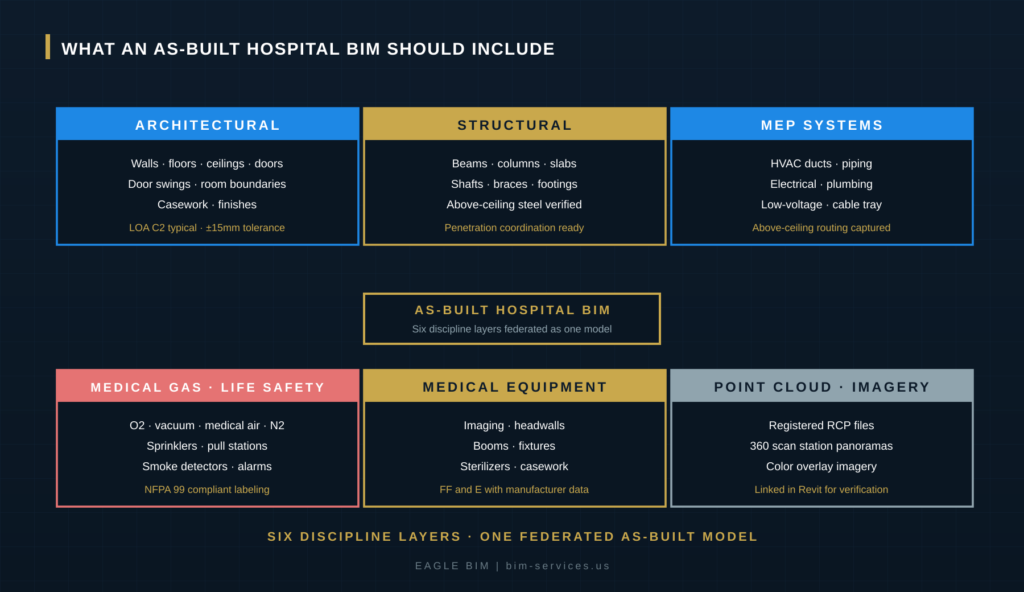
A complete as-built hospital BIM should include six layers federated into one model. Architectural: walls, floors, ceilings, doors, room boundaries, casework, and finishes. Structural: beams, columns, slabs, shafts, and verified above-ceiling steel ready for penetration coordination. MEP systems: HVAC ducts, piping, electrical, plumbing, and low-voltage routing captured in the plenum. Medical gas and life safety: O2, vacuum, medical air, N2, sprinklers, pull stations, and alarms with NFPA 99 compliant labeling. Medical equipment: imaging units, headwalls, booms, fixtures, sterilizers, and casework with manufacturer data. Point cloud and imagery: registered RCP files and 360 degree scan station panoramas linked in Revit for verification.
As-built hospital BIM is fundamentally different from a new-build BIM in that it has to be verifiable against the existing reality on demand. When the renovation design team has a question about whether a duct actually exists where the model shows it, they need to be able to click that duct in Revit and pull up the point cloud and the 360 degree scan station photo that captured it. This is why the registered point cloud and the spherical imagery have to ship with the model, not as separate deliverables.
Architectural and Structural Layers
Architectural capture in scan to BIM healthcare renovation has to include door swings, room boundaries with proper room naming and numbering matching the hospital’s facility management system, casework, and finishes. Standard commercial scan-to-BIM often skips door swings and detailed casework, but hospital renovations frequently touch these elements: code-required corridor widths, ADA clearances, infection control room layouts, and clinical equipment placement all depend on accurate door swing and casework data. The Level of Accuracy (LOA) target for hospital architectural scan-to-BIM is typically C2 (plus or minus 15mm) for general spaces, with higher precision in clinical zones.
Structural capture has to verify above-ceiling steel because renovation work routinely needs to penetrate beams, slabs, and shaft walls for new MEP routing. Older hospitals often have structural conditions that don’t match the original drawings. Steel locations move during construction. Slab penetrations close up over time. Shaft walls get rebuilt during prior renovations. The structural layer of the as-built model has to capture what’s actually there, with verified locations of every beam and column that could be in the path of upcoming renovation work.
MEP and Medical Gas Layers
Hospital scan to BIM MEP capture is the highest-value piece of the deliverable because renovation work overwhelmingly touches MEP infrastructure. HVAC ducts, chilled water and hot water piping, refrigerant lines, electrical conduits, cable tray, communication runs, sprinkler mains, and branch piping all route through the plenum and need to be captured in the as-built model. The Level of Accuracy for MEP scan-to-BIM is typically C2 for general routing and C1 (plus or minus 5mm) for specific tie-in points where the renovation design will connect to existing infrastructure.
Medical gas systems are a hospital-specific layer that standard MEP capture misses. O2, vacuum, medical air, N2, and N2O distribution all run through dedicated piping with NFPA 99 compliant labeling and source identification. The as-built model has to capture not just the piping routing but the source manifolds, zone valves, and alarm panels. The
NFPA 99 Health Care Facilities Code governs medical gas system installation and inspection. The §F§scan to BIM healthcare renovation§ deliverable should produce a medical gas model that the hospital’s facilities team can use for ongoing maintenance and that the renovation team can use to plan tie-ins and shutdowns without disrupting clinical operations.
Medical Equipment and Point Cloud Layers
Medical equipment capture covers fixed and semi-fixed equipment that the renovation work will need to coordinate around: imaging units (CT, MRI, X-ray, fluoroscopy), headwalls in patient rooms, ceiling-mounted booms in operating rooms and intensive care units, surgical lights, sterilizer rooms, and built-in casework. Each piece of equipment has clearance requirements, utility connections, and structural support needs that the renovation design has to respect. The as-built model should include manufacturer and model data wherever possible so the renovation team can pull spec sheets and clearance diagrams during design.
The point cloud and imagery layer is the verification spine of the entire deliverable. The registered RCP files contain every scan station’s data. The 360 degree spherical imagery (typically captured by the same scanner during the scan station) lets anyone working on the renovation design click any point in the Revit model and immediately see the photographic context. This is what makes as-built hospital BIM defensible: when the renovation team encounters something in the field that doesn’t match the model, they can pull up the point cloud and the imagery from the original capture to figure out what changed.
How Eagle BIM Delivers Healthcare Scan to BIM
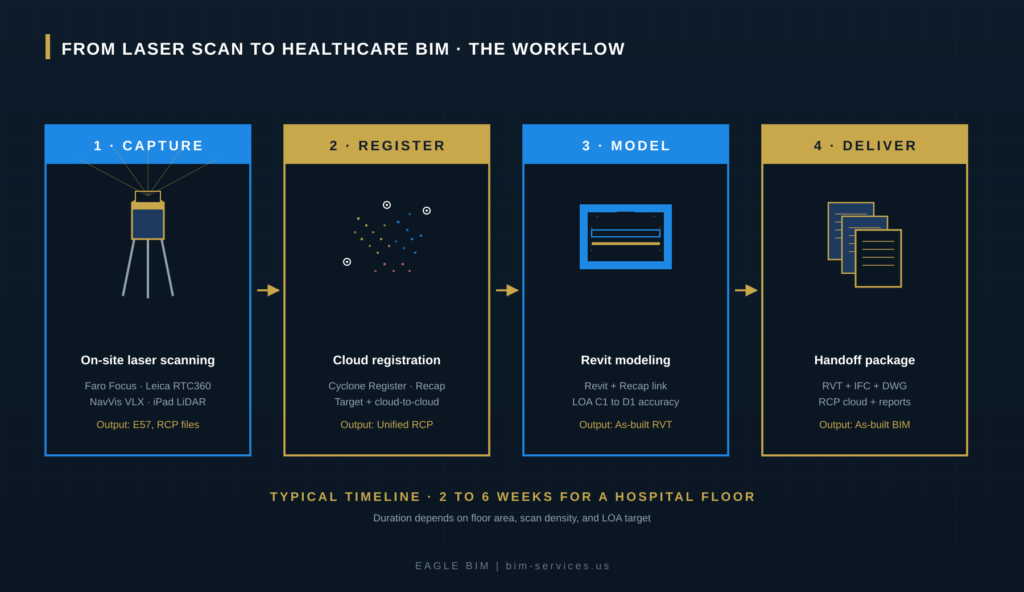
Eagle BIM delivers scan to BIM for healthcare renovation as a coordinated four-stage workflow: capture, register, model, deliver. Capture happens on site over a phased schedule coordinated with the hospital’s facilities and infection control teams. Registration consolidates the scan stations into a unified point cloud in Cyclone Register or Autodesk Recap. Modeling traces architectural, structural, MEP, medical gas, life safety, and medical equipment in Revit linked to the point cloud, typically at LOA C2 with C1 precision at tie-in points. Delivery includes the federated RVT model, IFC and DWG exports, the registered point cloud, scan station panoramas, and a verification document linking model elements to their source scans.
Our scan to BIM healthcare renovation engagements typically run two to six weeks per hospital floor, scaling with the floor area, scan density target, LOA requirement, and how much above-ceiling access is required. A typical 30,000 square foot patient floor with full MEP capture runs about four weeks from kickoff through delivery. A larger surgical floor with deeper equipment coordination might take six to eight weeks. We scope every engagement against the hospital’s renovation timeline so that the as-built BIM lands in the design team’s hands before they need it.
Eagle BIM works across Texas hospital systems including the Texas Medical Center campus in Houston, MD Anderson Cancer Center expansions, Memorial Hermann, Baylor Scott and White facilities, and Methodist Health System facilities across DFW and Austin. We also support healthcare GCs and design firms working in healthcare nationally. Our healthcare renovation modeling experience covers everything from single-floor med-surg renovations to multi-floor surgical platform expansions, imaging suite retrofits, and ED expansions. Each project type has its own scan-to-BIM nuances, but the underlying scan to BIM healthcare renovation workflow stays consistent: phased capture, ICRA discipline, federated deliverable. Our published
BIM for healthcare construction content covers our broader healthcare BIM workflow. The §F§scan to BIM healthcare renovation§ scope is one specific service within the larger healthcare BIM offering. Many of our engagements pair the scan to BIM work with downstream
MEP coordination services so the same team that captured the existing conditions stays on the project through the renovation design and construction coordination phases. The continuity reduces handoff loss and keeps institutional knowledge with the hospital’s renovation team.
Industry references for §F§scan to BIM healthcare renovation§ work include the FGI Guidelines for Design and Construction of Hospitals, the Joint Commission standards on renovation in occupied facilities, ASHE infection control guidance, and the NFPA 99 code on medical gas systems. Eagle BIM’s healthcare BIM team works to those standards as a baseline. The scan-to-BIM deliverable is part of the larger compliance ecosystem that hospital owners and GCs operate within, not a standalone capture exercise.
Texas-Specific Considerations for Hospital Scan to BIM
Texas hospital scan to BIM projects have specific local considerations. The Texas Medical Center in Houston is the largest medical campus in the world with continuous renovation activity across dozens of buildings. MD Anderson, Memorial Hermann, and Houston Methodist are perpetually renovating. DFW hospital systems including Baylor Scott and White, Methodist Health System, and Children’s Health are running major expansion programs. Austin’s healthcare sector is growing rapidly with Ascension Seton, St. David’s HealthCare, and Dell Seton expansions. Each of these systems has its own facilities management standards, BIM requirements, and ICRA protocols that scan teams need to know before they show up on site.
Texas climate also affects hospital scan to BIM work in a subtle way. The state’s heat and humidity put extra load on HVAC systems, which means hospital plenums in Texas tend to have larger chilled water lines, more aggressive condensate management, and more dehumidification equipment than equivalent facilities in cooler climates. Renovation work touching HVAC in a Texas hospital has to coordinate against this denser MEP infrastructure. The scan to BIM healthcare renovation deliverable for a Texas facility needs to capture these elements at higher fidelity than a generic commercial scan would.
Our published
Houston BIM coordination services covers our Houston-specific workflow including TMC project experience. The Texas Medical Center campus has its own institutional BIM standards that any scan-to-BIM team working there needs to understand before submitting deliverables. Eagle BIM has delivered §F§scan to BIM healthcare renovation§ work to TMC standards across multiple member institutions, which means our teams come pre-loaded with the standards rather than learning them on a first project.
Frequently Asked Questions
What is scan to BIM for healthcare renovation?
Scan to BIM for healthcare renovation is the process of capturing the existing conditions of an occupied hospital using laser scanners, then modeling those scans in Revit to produce an accurate as-built BIM that supports renovation design. The work happens under ICRA infection control protocols, scans during off-hours to avoid disrupting patient care, and captures architectural, structural, MEP, medical gas, life safety, and medical equipment data.
How long does scan to BIM take for a hospital floor?
A typical 30,000 square foot patient floor takes about four weeks end to end: one to two weeks for phased capture, one week for point cloud registration and QA, and one to two weeks for Revit modeling and deliverable preparation. Larger surgical floors with deeper equipment coordination can take six to eight weeks. Smaller outpatient zones can compress to two to three weeks.
Can you scan a hospital without disrupting patient care?
Yes. Phased capture scheduled around the hospital’s clinical operations is the standard approach. Patient floors scan after 10pm during the night shift when patients are sleeping. Surgical suites scan during scheduled cleaning windows or after the day’s case load. Outpatient and ambulatory zones can scan during weekend hours when activity is reduced. The entire approach is built around zero disruption to patient care.
What is ICRA and how does it affect hospital scanning?
ICRA (Infection Control Risk Assessment) is the protocol healthcare facilities use to classify renovation and construction activities by their infection risk to patients. Even non-destructive scanning falls under ICRA in clinical areas because the scan team is moving equipment through patient zones. Class III and IV areas require HEPA-filtered cart staging, dust barriers for above-ceiling work, disinfection between rooms, and tracked entry and exit logs. Every scan team working in healthcare has to be trained on ICRA protocols and operate under them throughout the project.
What level of accuracy does hospital scan to BIM target?
Level of Accuracy (LOA) C2 (plus or minus 15mm) is typical for general spaces and most MEP routing. LOA C1 (plus or minus 5mm) is used at specific tie-in points where new construction will connect to existing infrastructure. The USIBD Level of Accuracy Specification defines these tiers. Most hospital renovation work specifies C2 baseline with C1 at tie-in zones.
Does the deliverable include the original point cloud?
Yes. The registered point cloud (typically as RCP files for Recap) and the 360 degree scan station panoramas ship with the model. The point cloud is linked into the Revit model so the design team can click any element and immediately see the source scan data and photographic context. This makes the as-built model verifiable against the original capture, which matters when field conditions don’t match the model years later.
What software does Eagle BIM use for healthcare scan to BIM?
Capture hardware includes Leica RTC360, Faro Focus, NavVis VLX (for mobile scanning of corridors), and iPad Pro LiDAR for tight-access spaces. Point cloud registration runs in Cyclone Register and Autodesk Recap Pro. Modeling happens in Autodesk Revit with linked Recap point clouds. Output includes RVT, IFC, DWG, and the original RCP point cloud files for the hospital’s ongoing use.
Can you scan above existing ceilings without disrupting patients?
Yes, with careful coordination. Above-ceiling capture is typically done during the same off-hours scan windows as the rest of the work. The scan team removes ceiling tiles, deploys probe-mounted cameras or compact scanners into the plenum, and reinstalls tiles cleanly. In ICRA Class III and IV zones, dust containment and HEPA negative air filtration are required for tile removal. The work is fully coordinated with the hospital’s facilities team for tile access and reinstall.
| Ready to Scope a Hospital Scan to BIM Project?
Send Eagle BIM your hospital floor plan, renovation scope, and target schedule. We will come back with a phased scan to BIM healthcare renovation proposal that covers ICRA coordination, off-hours capture, MEP and medical gas modeling, and a federated as-built BIM delivery. Texas and USA coverage. |